
Back to DC HealthCare Alliance and Health Issues main page
|
Columns DCWatch
Archives Elections Government and People Budget issues Organizations |
NCMCNational Capital Medical Center July 12, 2005 ContentsI. Introduction and
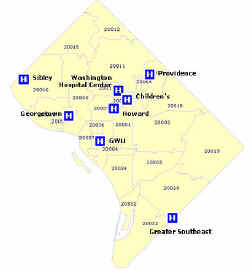
acknowledgements I. Introduction and acknowledgementsIn November 2003, Council proposed and passed emergency legislation directing the Mayor to negotiate an agreement with Howard University to build a new hospital on U.S. Reservation 13. In January 2004, the Mayor and the University submitted a Memorandum of Understanding (MOU) to Council. This MOU stated that the District would enter into a long-term lease with Howard University for 9 acres of land on U.S. Reservation 13. On that land, Howard University would build, own and operate a new 200 to 300 bed hospital with Level One trauma capabilities, a medical office building, and a research complex. The Council unanimously approved the MOU in May 2004. Since then, the District and Howard University have completed significant analysis, and the public has engaged in much discussion of the project. In the Fall of 2005, the Mayor will submit to Council for its consideration 1) An Exclusive Rights Agreement between the District and Howard University to govern the development of a hospital on parcels B and C on U.S. Reservation 13, and 2) a financing proposal and a grant agreement with Howard University to fund the District’s portion of the project. This report is a comprehensive joint proposal for the National Capital Medical Center (NCMC) prepared by the District of Columbia and Howard University. It is intended to provide the detailed information necessary for Council and the public to consider those requests. Any project of the magnitude of the NCMC requires several years of planning and architectural work prior to beginning construction--especially a project that is under the microscope of public opinion. This report represents the results of the initial phase of that planning effort. The first section provides the health policy context for the NCMC initiative and describes how the new medical center will fit into the larger healthcare delivery system. The next section explains the need for a full-service hospital on Reservation 13. Subsequent sections describe the NCMC’s planned programs, service area, size, operating costs, and the proposed relationship between Howard University and the District of Columbia. The report also includes preliminary architectural studies and financing plans. Contributors to this report include the following advisors to the District and Howard University: Goldman Sachs, HKS, Inc., The Lewin Group, Marshall Erdman & Associates, Perkins & Will, and Stroudwater Associates. II. Healthcare policy contextClosure of DC General Hospital and creation of a new healthcare visionFour years ago, Mayor Anthony Williams made the difficult decision to close DC General Hospital. The Administration, under pressure from the Financial Control Board, had no choice but to stem the large annual financial losses of the historic institution, which had served countless DC residents for decades. DC General had many positive attributes. Most notably, its services were available to anyone in need. As a result, it became a symbol of the District government’s commitment to DC residents. So it is not surprising that the hospital’s closure in 2001 outraged many District residents. But beyond curing the immediate financial woes of DC General, the Mayor envisioned remaking the District’s healthcare delivery system to promote improved health outcomes, not just to treat illness. Despite a $90 million annual DC General operating subsidy, the District had some of the worst health outcomes and highest hospitalization rates in the nation. The DC General Emergency Department—the gateway to healthcare for many District residents—was skilled at stabilizing and treating patients in the short-run, but not structured to provide prevention and long-term management of chronic illness. Moreover, DC General facilitated segregation of health services for poor African Americans. Mayor Williams proposed that the roughly $90 million annual DC General operating subsidy be spent instead on a new health coverage program called the DC Healthcare Alliance. This new program now provides comprehensive health coverage for District residents under 200% of the federal poverty level who are not otherwise eligible for the federal Medicaid program. In establishing this program, the District became the only jurisdiction in the U.S. to offer health coverage to all residents under 200% of poverty. As a result, the District’s uninsured rate is one of the lowest in the nation at just 9%1. And if every eligible District resident were enrolled, it is estimated that the District’s uninsured rate would fall to 4%.2 During the battle over DC General’s closure, many residents feared the worst, suggesting that “people would die in the streets” without the historic hospital. But four years later, it is clear that those alarmist predictions did not come true. In 2004, nearly 44,0003 District residents received health coverage through the DC Healthcare Alliance program, and another 138,0004 through Medicaid. By promoting primary care and ensuring that all Alliance enrollees have a Medical Home5, Alliance emergency department utilization dropped 29% and primary care physician utilization increased by 39% in 20046. In the poorest areas of the District, the rate of avoidable hospitalization trended downward for all age-groups, but especially for children.7 These encouraging statistics suggest that many low-income residents are now regularly seeing a doctor and getting preventive care rather that waiting until health problems become so debilitating that they require emergency care or hospital admission. Meanwhile, low-income patients in the District now have the choice of six different outstanding hospitals and many community health centers and private physicians, which are reimbursed for care that would have gone uncompensated in the past. The Alliance program, now in its fourth year, is in the process of being strengthened and improved to ensure its long-term stability and sustainability. It will be integrated into the Medicaid program to provide seamless coverage for low-income District residents. This reform effort is currently underway and will be complete by May of 2006.8 Four years after the closure of DC General Hospital, there is now broad consensus among District leaders in the Administration, Council, provider and advocacy communities to maintain comprehensive health coverage for all DC residents under 200% of poverty and to strive to expand enrollment to all those eligible for coverage. In addition, most District leaders have embraced the notion that all District residents should have choice of healthcare provider, and that low-income residents should not be systematically segregated from their higher income neighbors. Future vision for the healthcare delivery system in the District of ColumbiaDespite the major achievements of the District’s health coverage programs, the healthcare delivery system for low-income residents is still by no means perfect. Comprehensive health coverage is a necessary component of a strong system, but it is not sufficient. All District residents must also have convenient access to healthcare services, including primary care, diagnostic testing, specialty care, emergency care, trauma care, and inpatient care. Currently, these services are inadequately distributed across the District. Despite high health coverage rates, too many District residents in lower-income communities still report that they have no regular source of care9. And one must only examine the map of District healthcare providers to see that some areas of the District in most need, particularly neighborhoods in the Northeast and Southeast quadrants, are underserved. The Williams Administration is now pursuing two major initiatives to strengthen the private healthcare delivery system: Medical Homes and the National Capital Medical Center. Medical HomesMedical Homes will expand access to primary care and improve its quality. The initiative, in partnership with the DC Primary Care Association, the Brookings Institution, and many other organizations, will develop new and renovated community health centers to ensure that primary care is accessible in every community10. In addition, the new Medical Homes Certification Process will lead to improved quality of primary care and more sustainable business practices in District community health centers11. The Medical Homes initiative will improve health outcomes in DC by ensuring that all residents have access to a regular doctor who provides preventive care and helps them proactively manage their chronic illnesses. Over the next three years, the Mayor and City Council have committed $21 million in capital dollars toward this effort. In addition, they have approved $1.8M in fiscal year 2006 for operational support of Medical Homes. National Capital Medical CenterThe National Capital Medical Center (NCMC), a new medical complex owned and operated by Howard University, will become a hub for the community health system on the Eastern side of the District. It will address the problem of access to specialty care by housing a medical office building which will attract specialty physicians to provide consultation for serious medical conditions. It will provide a much-needed referral point for diagnostic testing that requires major medical equipment. It will improve access to emergency and trauma care for residents in the Northeast and Southeast quadrants, who must now endure ambulance trips that are sometimes dangerously long. In addition, it will alleviate overall pressure on the District’s emergency medical system, which experienced more than 7500 hours of emergency department closure and diversion in 2004. The balance of this report describes the District and Howard University’s proposal for the National Capital Medical Center. III. Need for a full-service hospital on Reservation 13Over the past eighteen months, The District and Howard University have engaged in numerous studies and analyses to determine the extent to which District residents would be well-served by a hospital located on the site of U.S. Reservation 13. The results of this work are clear. There is an authentic need for a hospital of roughly 250 beds that provides a comprehensive array of health services, serving primarily residents of Wards 5, 6 and 7. The National Capital Medical Center (NCMC) is needed for four major reasons: 1) to create a better geographic distribution of hospital services, 2) to increase overall capacity, especially for emergency care, 3) to serve as a hub for the community health network in Northeast and Southeast, and 4) to disperse the current clustering of District hospitals, which could be problematic in the event of a major disaster. Need for better geographic distribution of hospitalsWhen the Council first enacted the “National Capital Medical Center Negotiation Emergency Act” in November 2003, the legislation noted that “the District’s existing healthcare infrastructure is inadequate in part because of the uneven distribution of hospitals throughout the city.” Since then, much research has been completed to confirm this statement. The District’s hospital facilities are predominately concentrated in the central and western areas of the city, with just one hospital east of the Anacostia River in Ward 8. Location of Major Acute Care Hospitals in the District
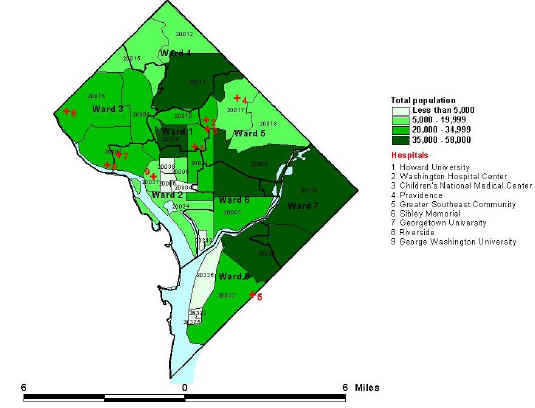
However, much of the need for healthcare services in the District is in areas that are not proximate to a hospital. Many of the most densely populated neighborhoods are located in Northeast and Southeast. Population Density and Location of District Hospitals
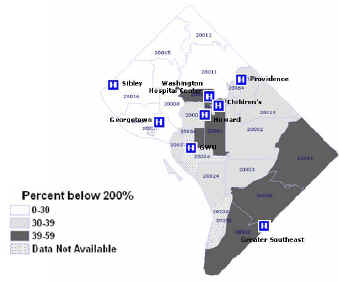
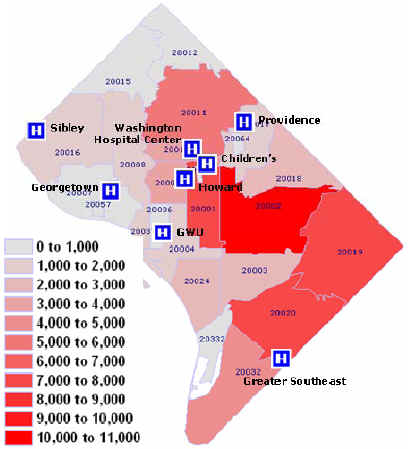
Source: Applied Graphic Solutions and US Census Moreover, these densely populated neighborhoods without easy access to a hospital are highly concentrated with the District populations who are most in need of medical services, such as residents below 200 percent of the federal poverty level, residents covered by Medicaid and the DC Healthcare Alliance, African-Americans, women of childbearing age, and children. Location of Low-income Residents and District Hospitals
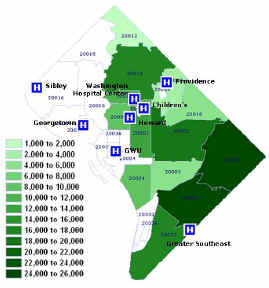
Source: 2000 U.S. Census Bureau Location of Medicaid and Alliance Members and District Hospitals
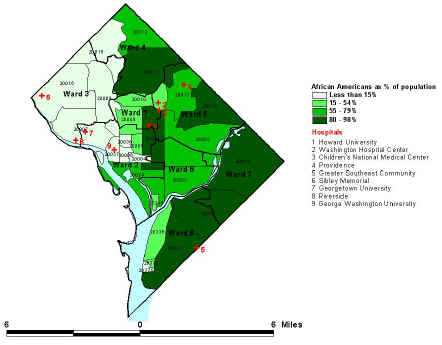
Source: Healthcare Safety Net Administration and Income Maintenance Administration Location of African American Population and District Hospitals
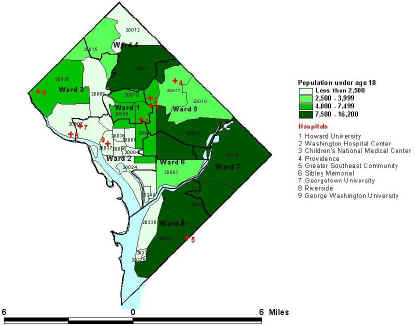
Source: 2000 U.S. Census Bureau Location of Children Under Age 18 and District Hospitals
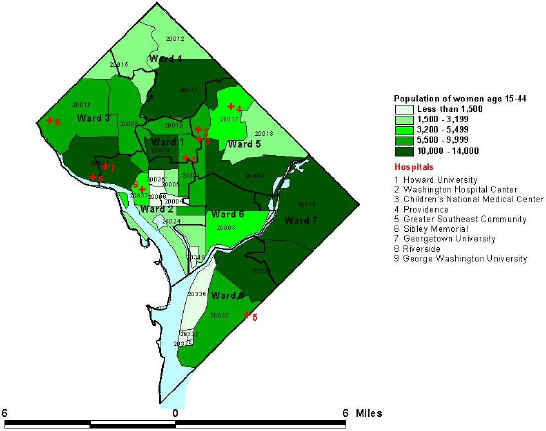
Source: 2000 U.S. Census Bureau Location of Women of Childbearing Age and District Hospitals
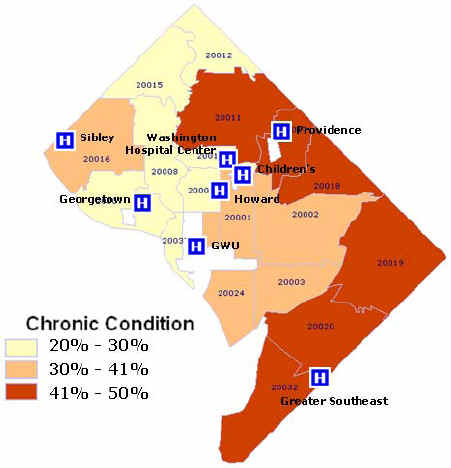
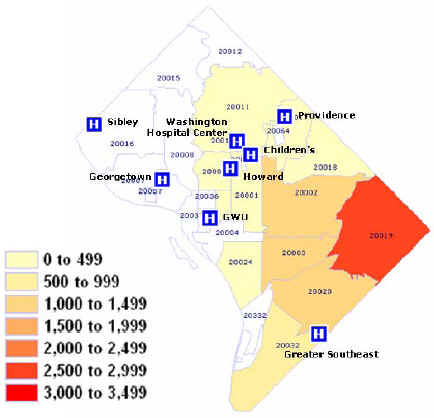
Source: 2000 U.S. Census Bureau In a recent study commissioned by the DC Primary Care Association, the RAND Corporation quantified the burden of chronic illness in different parts of the city. The results of that study show that many of the areas with the highest concentrations of chronic illness are also in areas without a hospital. In these neighborhoods, as much as 50% of the population has Diabetes, Asthma and/or hypertension. Location of Chronic Disease Burden and District Hospitals
Source: RAND Corporation Analysis sponsored by DC Primary Care Association The mismatch between the need and the location of services is particularly pronounced for emergency and trauma services. In 2004, 27% of all District EMS calls came from areas east of the Anacostia River, where there are no trauma services and only one emergency room at Greater Southeast Community Hospital, which is on the Southeast border with Prince George’s County. Another 22% of EMS calls came from areas just west of the Anacostia River, near Reservation 13. Major traffic congestion between these locations of need and the District’s existing hospitals can compromise the health of patients who must be transported long distances to receive care in life-threatening circumstances. Origin of EMS Ambulances and Location of District Hospitals
Source: District Fire & EMS In the past, many of the residents of these now underserved communities relied on DC General Hospital. Over three-fourths of DC General patients came from zip codes 20001 (Ward 2), 20002 (Ward 5), 20003 (Ward 6), 20019 (Ward 7), 20020 (Ward 6), and 20032 (Ward 8). Origin of DC General Patient Discharges
Thus, the areas of the city with the highest concentrations of people needing healthcare services—the poor, African-Americans, women of child-bearing age, children, and the chronically ill—are the least accessible to key health services. Residents of these underserved neighborhoods must travel across the city for emergency and trauma care, inpatient care, surgical procedures, and diagnostic tests. And because specialty physicians tend to practice in close proximity to hospitals, they must also frequently travel to see a doctor. Need for additional capacityIn addition to a need for redistribution of hospital services, the District is also likely to have a need to expand total hospital capacity in the coming years. Statistics from around the country show that after more than a decade of hospital consolidations and declines in the number of beds, the need for hospital services is now increasing. In the 1990s, the number of beds in the U.S. sharply declined due to dramatically reduced lengths of stay and a major shift from inpatient to outpatient procedures. These changes were largely due to advances in minimally invasive technologies, a new Medicare payment methodology, and the pressures of managed care. In the 2000s, new trends such as the aging of the population, different medical technology advances, and the relaxation of managed care practices are gradually increasing the need for hospital services nationwide. US Hospital Volume Trends
The District of Columbia is beginning to see similar trends, and may soon or already need additional ER (Emergency Room) capacity and operating hospital beds. One way to evaluate whether the District’s current ER capacity is sufficient to meet the demand is to examine the number of hours of ER closure and diversion at District hospitals. Hospitals frequently ask District EMS to reroute ambulances to other facilities when their ERs are at capacity or when the number of open beds in the adjoining hospital is not sufficient to accommodate more very sick patients. The number of hours of diversion and closure more than doubled over the past five years, from 3599 hours in 2000 to 7515 hours in 2004. This suggests that there is indeed a need for additional ER capacity. In addition, it appears that after years of decline District hospitalizations may be on the rise. The number of staffed acute care beds in the District declined by 476 in recent years with the closures of DC General and the Columbia Hospital for Women and the conversion of Hadley Memorial to a long-term care facility. In addition, all remaining District hospitals currently operate far fewer beds than their licenses allow. During the fourth quarter of 2004, the total number of licensed DC acute care beds was 3914, with only 2651 beds were in operation.12 But the number of total acute care admissions is now slowly increasing in the District. Number of District Acute Care Admissions, 2000-2004
Source: DC Hospital Association As a result, after years of decline, the need for hospital beds is likely to grow in the near future, mirroring national trends. Our analysis suggests that if the District population and the rate of hospitalization were to remain stable, by 2008 the District would require another 349 operating beds. If the District population were to grow by 23,500 (half the growth projected by the Office of Planning) and the rate of hospitalization declined somewhat, by 2008 the District would require an additional 218 operating beds.13 Some might argue that existing hospitals could fill the increasing need for beds and emergency care by opening inpatient wards that they have closed over the years and expanding the size of their emergency rooms. However, given the stark mismatch between the location of existing services and the areas of predominant need, a strong case can be made that any new operating beds should be located in the areas of greatest need, on the Eastern side of the District. Reservation 13 is an ideal location, given its proximity to major transportation thoroughfares and historical healthcare context. Need for a community health network hub and key public health servicesThe east side of the District is in need of a major medical facility to anchor the developing community health network. There are currently some primary care providers located in these underserved areas--community health centers and private physician practices that focus prim primarily on the publicly insured and uninsured populations. This network is poised to expand and improve as the Medical Homes initiative progresses. However, these community providers are often stymied in their goal of providing adequate care for their patients because of a lack of available specialty physicians to provide consultations and no readily available referral point for major diagnostic testing. Frequently, these providers are forced to tell their patients to travel across the city to a hospital emergency room to seek these services, since there are no local facilities to which they can proactively refer patients. As a result, many patients do not receive necessary care, or they receive care inefficiently, in a hospital ER. A new medical center on the Reservation 13 campus could serve as a referral point for community providers seeking specialty and diagnostic services for their patients. Through formal referral agreements and information technology connecting hospital providers, a new medical center can provide the missing link in the current continuum of care. Need to disperse the cluster of hospitalsIn addition to correcting this mismatch between the location of existing facilities and the everyday demand for services, Washington, DC must also consider the implications of hospital location in the event of a major disaster or breach of homeland security. In such an unfortunate situation, it will be crucial for District health delivery services to be spread out across the city, so that if hospitals in one area are affected, others can continue to provide life-saving services. However, we currently have a major cluster of hospitals in a vulnerable location in the center of the city. Washington Hospital Center, Children’s National Medical Center, Howard University Hospital, the Veteran’s Administration Hospital, and Providence Hospital are all in very close proximity to one another. Moreover, the three Level One Trauma Centers in the District, Howard University Hospital, Washington Hospital Center and Children’s National Medical Center, are all within a mile of each other. If all of those hospitals became incapacitated at the same time, or if residents from the East side of the District could not reach them, lives would be lost. The District’s emergency and trauma capacity must be better distributed across the city, both for better access on a daily basis, but perhaps more importantly, for access in a crisis situation. It is clear that a new hospital on Reservation 13 would fill the current gap in services in the District. The remainder of this document describes in detail a joint proposal of Howard University and the District government for the National Capital Medical Center, a hospital that would meet the needs described above. IV. Overview of the National Capital Medical and key servicesVisionThe establishment of the National Capital Medical Center (NCMC) on Reservation 13, as a modern, comprehensive, state of the art tertiary medical center, with Level One trauma, in alliance with community physicians and clinics has great potential to enhance the delivery of healthcare services for the benefit of a significant portion of the District’s population. The NCMC will provide a single standard of high quality, world-class comprehensive care for all, without regard to ability to pay. The vision for the NCMC includes the following elements:
The National Capital Medical Center will be an integrated medical complex containing three major components: a hospital, a medical office building, and a research center. The medical center will also provide additional services for the surrounding community. Public health services will be offered within the complex or in close proximity. The NCMC will serve as a major hub for the community health network. HospitalThe hospital will be a primary teaching facility for the Howard University School of Medicine. As such, it will provide tertiary-level services. Departments will include:
The hospital will provide four major types of beds for acute inpatient care: medical/surgical, obstetrics and gynecology, pediatric, and psychiatric. It will also include a secure unit with a separate entrance for corrections patients. The NCMC will participate in the new Department of Mental Health program to care for involuntary, acute mental health patients. The NCMC will include a sizable 24 hour, 7-day a week emergency and trauma service, with capacity for a minimum of 50,000 emergency room and approximately 4,000 trauma visits. In addition, the NCMC will provide other outpatient diagnostics services such as radiology and laboratory. Community-based physicians will be able to refer their patients for these diagnostic services. Medical office buildingA medical office building adjoining the hospital will house community physicians. These physicians will provide outpatient primary care and specialty care to community residents. They will admit patients to the NCMC and use the NCMC procedure rooms. Community-based practitioners will be able to refer patients to NCMC-based specialists for consultation. Research centerThe NCMC will also develop facilities and services on its campus as a continuum of its public health, research, and education mission. Major research programs may include Aging, Clinical information systems, and Nursing. Other community servicesIn addition, the NCMC will offer and provide an array of services as a community benefit, to improve the quality of life for area residents. Such services may include:
Community health network for underserved populationsThrough thoughtful, well -planned services, the NCMC expects to significantly increase accessibility of the full continuum of care to underserved District populations. This will allow a currently underserved population to access the level of care appropriate to their need, whether it be primary and preventive care, specialty services, diagnostic and ancillary services, urgent care or emergency services. The NCMC will offer wellness, prevention and an array of services that contribute to healthier lifestyles and positive health outcomes, particularly for those diseases and conditions that are highly prevalent within minority communities. Services will include nutrition counseling, support groups, physical fitness classes and other related programs aligned with the public health and prevention research focus of Howard University. A number of public health services have traditionally been offered on Reservation 13 (the former DC General site). These services, specifically a tuberculosis clinic, an STD clinic, a detoxification center and a primary care medical home will continue to be offered within close proximity of the NCMC. These services will be provided by the District Government or contracted out to the NCMC or other community providers. In addition, the NCMC will work with several community health groups to eliminate health disparities through provision of primary and secondary preventive services designed to reduce ambulatory sensitive hospitalizations and to improve outcomes of those systemic conditions that adversely impact the surrounding population. Specific initiatives will include:
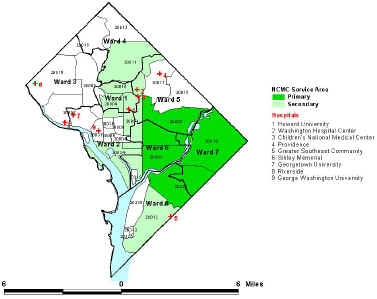
Serving as the hub of a well-coordinated care delivery system, the NCMC will provide specialty, diagnostic, urgent and emergency care to meet the needs of Medical Homes primary care patients. Howard University Hospital and the NCMCHoward University Hospital and the NCMC will become a two-campus healthcare system under unified governance. The coordinated approach will provide high quality healthcare. The proposed organizational structure will maximize efficiency and use of resources. The services that Howard University plans to offer at the NCMC are based on the needs of the community. The greatest unmet need is for Level One trauma care. Therefore, the University will consider moving its Level One trauma and requisite related services--neurosurgery, cardiovascular surgery, and orthopedic surgery-from Howard University Hospital to the NCMC. Given the current proximity of the University’s pediatric and adolescent services to Children’s Hospital, the University will also consider moving these services to the relatively underserved area where the NCMC will be located. The Level III NICU (Neonatal Intensive Care Unity), which supports the obstetrics service, may also be relocated. V. Service area, projected volumes, and bed requirementsHoward University contracted with a nationally recognized healthcare consulting firm, The Lewin Group, to determine the size and scope of the National Capital Medical Center (NCMC). Lewin completed a detailed market study that required analysis of the demographic profile and the utilization patterns of all patients treated by acute care hospitals in the District of Columbia. This analysis yielded assumptions about the NCMC’s service area, projected service volumes, and need for beds. A similar analysis, completed by District consultants Stroudwater Associates, confirmed this analysis. NCMC Service AreaAssumptions were made regarding the NCMC’s service area, based upon historical utilization patterns of residents, changes in demographics, and other factors that might impact service area demand. Hospitals typically draw the greatest share of patients from residents proximate to the medical center campus. For planning purposes, the geographic origin (zip codes) from where a hospital derives 80-85% of its discharges defines its core service area. Given an understanding of care-seeking patterns and the location of the new hospital, Lewin defined zip codes within Wards 1, 4, 5, 6, 7 and 8 as the core service area of the NCMC. This area encompasses the primary service area, shown in dark green below and the secondary service area, shown in light green. Projected NCMC Service Area
NCMC Service VolumesTo determine the volume of services likely to be provided at the NCMC, The Lewin Group first identified the entire potential “pool” of District hospital discharges using inpatient hospital patient discharge data by zip code, payor and service groupings. This analysis projected 143,000 total hospital discharges in the District of Columbia. The following chart breaks out those projections by the NCMC service area and bed type. DC Hospital Projected Discharges by Bed Type
Then, assumptions were made about the market share of the NCMC, given historical area wide patterns of utilization. Lewin made assumptions regarding the likelihood of the NCMC recapturing market share of residents who formerly used DC General, and the likelihood of the NCMC gaining new market share in the primary service area, secondary service area, and areas outside of the District. Key assumptions include:
These assumptions yield the following projected market share: NCMC Projected Market Share
Applying these market shares by service yielded the following projected inpatient volumes for the NCMC. NCMC Projected Discharges
NCMC Projected Key Statistics by Major Bed Type
Estimated Bed Need by Type and Occupancy Rate
NCMC Admissions
EMS trauma-run data indicates a substantial number of trauma patients reside in the southeastern quadrant of the District. Because the NCMC would be located close to a major or high way, the trauma center is ideally located and will likely generate volume from outside of the immediate area. Emergency room demand is tied most closely to geographic proximity, and the area surrounding the hospital is among the most densely populated in the District. In 2002, average emergency room visits at each of the District’s three trauma hospitals and at Greater Southeast equaled 51,000. Patient care provided in an ambulatory care setting is trending upward in the District and nationwide. NCMC Projected Volumes for Ambulatory Care Services
VI. Physician staffingThe success of the National Capital Medical Center (NCMC) is dependent on attracting a strong provider network that will refer patients to the NCMC facility for procedures and admissions. We estimate that the NCMC will require approximately 217 full time equivalent physicians (FTEs) based on patient demographic characteristics and insurance status , and physic physician productivity. Since many community physicians admit to more than one hospital, the total number of affiliated physicians will need to be greater. Projected Physician Demand in FTEs for NCMC Year Three
It is estimated that the number of community physician FTEs needed for the NCMC would range from 80-100. The University is well poised to build the physician network that is needed to support the population served by the NCMC for the following reasons:
VII. Conceptual site and facility designSiteThe proposed site for the National Capital Medical Center (NCMC) is on the Northeast corner of U.S. Reservation 13, just south of RFK stadium and just west of the Anacostia River. The site sits between major centers of population on both sides of the river and is adjacent to key transportation routes, including bridges, highways, and the Stadium/Armory Metro station. Location of the National Capital Medical Center
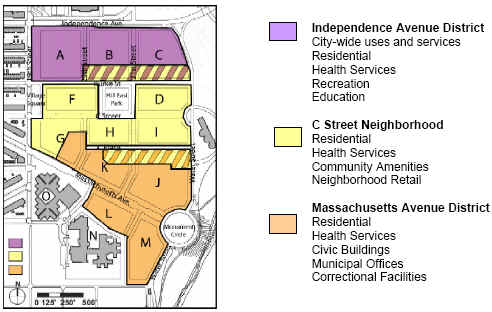
Reservation 13 is currently home to the campus of the former DC General Hospital, as well as the DC jail. From the time of the origin of the L’Enfant plan to today, the area has been an isolated campus separate from the rest of the city. In 2003, the District of Columbia Office of Planning led a major planning process, including 15 government agencies and more than 300 citizen stakeholders, to create a Master Plan for the redevelopment of Reservation 13. Out of this process emerged a new vision for the site, as a beautiful public place that links the existing neighborhood to the waterfront while also meeting District-wide needs for healthcare, recreation, civic space, and housing. Reservation 13 Master Plan
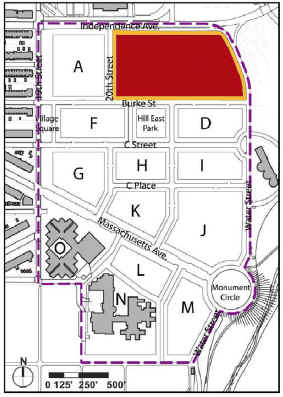
The proposed site for the NCMC is located on the Northeast comer of Reservation 13, on sites B and C in the Independence Avenue District. This parcel of land totals roughly 9 acres. Location of NCMC on Reservation 13
The NCMC and all Reservation 13 developments will be consistent with this Master Plan that was developed in consultation with the community and approved by the Council. The Reservation 13 Small Area Plan has been adopted by the City Council as a clarification to the District's Comprehensive Plan. The Office of Planning has since set down with the Zoning Commission draft zoning for the site, which includes detailed design guidelines and a special exception review requirement. Any building project on the site will be subject to zoning. Concept facility designHoward University engaged the services of Perkins & Will/Marshall Erdman & Associates to conceive a design concept for a state-of-the-art medical center situated on Reservation 13. The design team created a conceptual space program based on its experience with similar projects. All designs are preliminary and will become more detailed after consultation with the community and the completion of a detailed functional space program, which will specify every room needed in the facility, including square footage and functional requirements. The conceptual space program includes four major components:
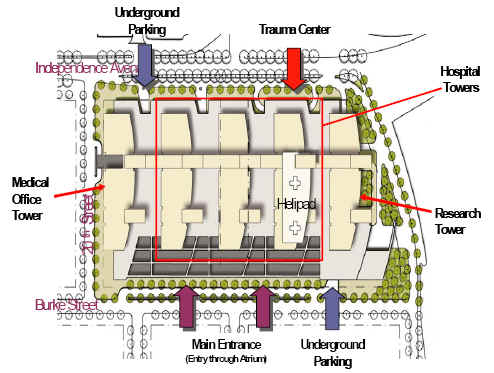
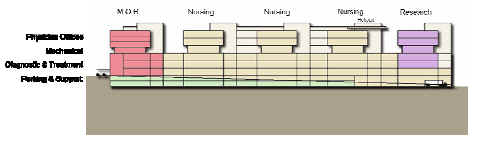
The three components will have one campus-wide infrastructure, which will optimize investment. The medical office building will be integrated into the hospital facility with a dedicated entry at the western side of the campus along 20th street. Construction for all acute care facilities on the campus will be "Type I" (Institutional Occupancy). All rooms will be private, with the opportunity to expand capacity to double or triple occupancy in the event of surge in demand due to a major disaster. Ambulatory care facilities will also be developed to an Institutional Occupancy standard to accommodate flexibility for future undefined programs or services. Build-out and finish selections for the medical office building will be to a "Type B" (Business Occupancy) standard to approach the tenant cost per square foot of other similar facilities in the area. Structured parking will be constructed in a maximum of 3 levels below ground to avoid water table restrictions. The facility will utilize separate circulation systems for public and support functions to optimize customer perception and operating efficiencies. Public circulation systems will be designed to integrate intuitive wayfinding and orientation with directional signage and interactive computer map kiosks throughout the campus. Support circulation systems (such as supply routes, waste removal and staff routes) will be concealed from public view and access for both positive image and to avoid functional conflicts. In addition, flexibility will be optimized through modular facility design, a campus circulation grid, and shell space. A nominal 30'x30' structural grid optimizes flexibility for current delivery of care standards and room dimension modules for examination room, nursing beds, ICU and diagnostic & treatment procedural platforms throughout the facility. The proposed 17' floor to floor height provides sufficient plenum space to accommodate engineering systems and the growing intensity of data communication systems to support medical equipment. Given its urban location adjacent to neighborhoods, the river, RFK stadium, and the armory, the NCMC is unlikely to have an opportunity to grow beyond the 9acre boundaries of the proposed site in future years. Therefore, the conceptual design incorporates some space that can be used for expansion of hospital services. Campus Conceptual Plan
Conceptual Cross Section
The proposed NCMC development will contribute to the new Hill East neighborhood in several ways. The large building program will be broken down into smaller, discrete elements to complement the residential scale and integrate with the proposed adjacent commercial retail zoning. An inviting Atrium Lobby will be located on Burke Street with public access to food, retail and educational services. A public park will be developed on the roof of the sub-grade parking at 21st Street between Burke Street and C Street, creating a focal point for neighborhood activity. The NCMC will serve as a transition between the high traffic volume of Independence Avenue as well as the public scale of the RFK Stadium and the Armory to a quieter, comfortable neighborhood scale. The architectural character will support the proposed neighborhood guidelines for building materials and color palette to integrate with the character of the overall community concept. The pedestrian experience to the west and south will be enhanced through detailed groundscape and an articulate way-finding system, while the Independence Avenue facade provides an inviting vehicular gateway and screen for the overall residential scale of the neighborhood. Within the Atrium a variety of flowering plants and trees will flourish and embrace the character of the neighborhood park to the south. The Atrium will provide a year-round setting for casual conversation and public health education. Several retail shops will be accessible from the Atrium such as a coffee shop, pharmacy, convenience store, bank, fitness center, and post office. Conceptual rendering of the NCMC
The National Capital Medical Center is an extremely important and complex project. It will require careful planning, including extensive community input, to ensure that the facility meets the needs of the community for the long term. A project of this complexity requires many steps that must be completed in sequence. An accelerated project schedule is being developed to build the National Capital Medical Center as quickly as is feasible. The elements of the NCMC schedule include preliminary planning and programming, demolition and preparation of the site for construction, architectural design, and construction. Facility planning and programming has already begun. Site preparation will begin shortly, now that Council has approved $6 Million to begin demolition and utility work. It will include building demolition, hazardous material remediation, site demolition, site grading, new street construction, metro and streetscape improvements, and park improvements. VIII. District and University roles and responsibilitiesThe National Capital Medical Center (NCMC) is a public/private partnership between the District of Columbia and Howard University. The NCMC will be built, owned and operated privately by Howard University, but given the demonstrated need for this new institution to provide medical services to underserved District populations the District will provide resources for its development and construction. FinancingThe District will contribute nine acres of land on the Northeast corner of Reservation 13 for the hospital, through a 99-year, one dollar per year ground lease. The land was valued in the range of $50 to 70 million in mid-2004. The District has agreed to provide up to 50% of the hospital capital costs for the new medical center. In addition, the District will cover the costs of basic infrastructure development on the hospital site, including demolition of existing buildings, environmental remediation, site grading, and extension of the street grid. This infrastructure work is currently estimated to cost roughly $30 to 35 million in today's dollars. The District will not provide any direct operating subsidy at startup or over the life of the institution. Howard University will fund the balance of the project costs through outside federal or private grants, equity, and/or private debt. Howard University will pay the debt service on any debt for this portion of the financing with no obligation of the District. GovernanceHoward University will incorporate a new nonprofit organization that will own and manage Howard University Hospital and the National Capital Medical Center and coordinate programs between the two facilities. Members of the Board of Directors of the organization will be selected by Howard University and the Mayor. Development processThe University will be responsible for all healthcare planning, business planning, architectural design, and construction of the NCMC. It will hire a construction project management firm with experience managing hospital construction projects, in consultation with the District, to manage all aspects of project. The University will be responsible for developing and awarding all RFPs, in consultation with the District. The District (Anacostia Waterfront Corporation), in consultation with Howard University, will be responsible for planning and implementation of infrastructure development, including demolition, environmental work, grading, and new street construction. The District will deliver the site ready for hospital construction by the end of the Predevelopment Phase. Howard University commitmentsHoward University has committed that the NCMC will work with the District to promote public health by creating a continuum of care for underserved residents, reducing unnecessary emergency room visits and avoidable hospitalizations, serving the District in the event of a disaster, and providing care to District residents regardless of their ability to pay. Prior to construction of the NCMC, the University will develop public health operating plans in consultation with the District that describe how the NCMC will meet these goals. The NCMC will also report annually on its public health activities. In addition, the University has agreed that the NCMC will provide space and/or management for key public health services, if required by the District. These services may or may not be located at the NCMC, but will be located in areas of greatest need and with reasonable proximity to the NCMC. Such services could include public health clinics, mental health/substance abuse crisis services, involuntary acute mental health services, secure services, and public health outreach. In addition, the NCMC will make a strong commitment to the people of the District of Columbia by employing District residents to the greatest extent possible. It will also contract with small local businesses because these businesses make a significant contribution to the local economy through job creation and business expansion. Project Deliverables and Funding PhasesNCMC development will proceed in three phases: Planning, Predevelopment, and Construction. Howard University will be responsible for all deliverables (except initial infrastructure and site work). The District will have the right to participate in the planning process, and Howard will give the District the opportunity to approve major deliverables. Planning phase Estimated timing: 6 months
Pre-development phase Estimated timing: 12 to 18 months
Construction Phase Estimated timing: 24 to 36 months Performance standards and remediesDuring the planning and construction phases, Howard University will provide the District with all deliverables within the timeframe that has been mutually agreed upon, including initiation and completion of construction of the facilities. The University will also provide audited financial statements within 120 days of the end of each fiscal year of the project during the planning and construction phases and once the NCMC is operational. Howard University will also annually report on compliance with all bond covenants for debt. Howard University will maintain a license to operate an acute care facility in the District of Columbia, any licenses needed to operate a physician's office building and related services, and all relevant accreditations, including JCAHO, required for Medicaid and Medicare reimbursement. Howard University will annually report the NCMC's uncompensated care policy and the volume of care provided as uncompensated care. It will also report on all public health and required services that it is providing. It will report on its compliance with all relevant District or federal quality standards. Failure to comply with the any of the terms of the agreement or failure to report on those terms may be grounds for termination of the long-term ground lease. AgreementsThe provisions described above will be formalized through several legal agreements between the District Government and Howard University:
IX. Projected operating financials and key success factorsIn order to determine the feasibility of the NCMC and its ability to meet the healthcare needs of residents of the District of Columbia in future years, Howard University prepared a series of financial statements and analyses. The University consulted with The Lewin Group, Perkins & Will/Marshall Erdmann & Associates, and Goldman Sachs to assist in estimating the volume of services, construction and related project costs, and financing options that would help inform the financial pro forma statements as well as the capital requirements during pre-opening years. The following represent the key assumptions underpinning the forecasted financial statements:
Based on the financial forecast, the NCMC should break even during the third year of full operation. During the first two years of operations, the NCMC will incur losses of $13.4 million and $3.9 million, respectively, as the delivery system recovers from the fixed costs of opening a new facility. Year three represents the "hurdle" year of operations, when growth in admissions, ambulatory, and ancillary services will increase net patient revenue and other revenue to the point that they exceed operating and capital costs. Patient volumes reflect the vision of the NCMC to be recognized as the premier healthcare provider in its service area, to develop strong relationships with physicians, and to coordinate with a network of health service providers throughout the District, thus expanding its referral network. To estimate revenue streams, the financial pro forma include assumptions regarding the payor mix (patient's type of insurance coverage). The NCMC will be attractive to all residents, including those with commercial and public sources of insurance, and consistent with its mission, will serve a substantial number of patients who are uninsured or underinsured. The financial forecast assumes that 39% of patients will have private insurance and 61% will have a public source of insurance, held constant for all five years. On a comparative basis, the projection reflects a greater proportion of commercial and Medicare mix than was historically served by DC General and a greater proportion of self-pay and charity patients than all other District hospitals with the exception of Howard University Hospital. NCMC Probable Payment Source
Given that the NCMC will be a tertiary service provider, patients seeking services will have a higher acuity, or case-mix index (CMI). The forecasts assume that the CMI for Medicare and Medicaid patients will be 1.62 and 1.49, respectively. This assumption is held constant for all five years of the financial forecast. In addition, given the patient population, the forecasts assume the hospital will become a disproportionate share hospital (DSH) and receive Medicaid DSH funds. Howard University Hospital's experience forms the basis for labor and non-labor expenses (see exhibit on operations assumptions and exhibit on key financial ratios). Staffing levels in the forecasted financial statements take into account the mix of services that the NCMC will offer and Howard University Hospital's salary and benefits costs per full time equivalent (FTE). During year one, the forecast assumes staffing levels of 5.0 FTEs per adjusted occupied bed (AOB), which will decrease in future years to 4.8 FTEs per AOB as volumes increase and the hospital operates more efficiently. The forecast assumes that physician expenses, pharmaceuticals, and all other medical supplies will vary based on the number of patient days. Note that the forecast reflects costs in today's dollars. NCMC 0perations Assumptions
The following exhibits represent detailed financial statements forecasted for the NCMC for the twelve-month period ending June 30 for years one through five of operations. The presentation of the statements is in thousands of dollars with the exception of the key financial ratios. NCMC Forecasted Statement of Operations(Dollars in Thousands) I. FOR THE TWELVE MONTHS ENDED JUNE 30II.
NCMC Forecasted Statement of Cash Flows(Dollars in Thousands) B. For the twelve months ended June 30
NCMC Forecasted Balance Sheet(Dollars in Thousands)
Key Financial Ratios
Critical success factorsGiven the history of financial difficulties at DC General, the NCMC's financial viability will be closely tracked. Both the University and the District recognize that it will be a challenge to operate the NCMC. profitably. Every hospital in the District of Columbia and most hospitals nationwide face this same challenge. However, with careful planning, successful relationship building, and the implementation of critical strategies, the District and the University believe the NCMC will be successful. To ensure profitability, the NCMC must balance its patient base along a number of dimensions. It must draw a payor mix that roughly mirrors the population of its service area. To do this, it must offer programs, staffing, and facility accommodations to meet the expectations of both private and publicly insured patients. The NCMC must also draw a substantial number of higher acuity patients, especially surgical patients, who generate higher reimbursements per bed. The development of a Level One trauma center and related centers of excellence will promote this goal. The NCMC must also attract and retain a high-quality medical staff that earns a reputation for excellence in tertiary medical care. This requires drawing upon the strengths of academic medicine, utilizing Howard University faculty and residents, as well as developing relationships with private, community-based physicians to provide healthcare to greater numbers of commercially insured District residents. To do so requires development of a medical office building, in addition to the hospital, that can be used by physicians to provide outpatient diagnostic care and procedures for their patients. In addition, the NCMC must strive to operate according to national benchmarks. It must manage its cost per discharge, consistent with quality care. And it must manage its revenue cycle and collections process. The NCMC's efficient facility design, electronic patient records, and state-of-the-art medical equipment will promote these efficiencies. In addition, as a two-hospital system, Howard University Hospital and the NCMC can consolidate some services at either campus to maximize efficiency while meeting community healthcare needs. X. Project costs and financing Project CostsHoward University engaged the services of Perkins & Will/Marshall Erdman & Associates to create a conceptual framework for a state-of-the-art hospital that would conform to the designated nine acre space reserved for the NCMC on Reservation 13. They also provided cost estimates based on their experience and industry standards for healthcare facilities similar to the type and scale of the NCMC. Using space and unit cost benchmarks, they estimated that the hospital facility project would cost approximately $400 million in today's dollars. This cost estimate is expected to increase as planning progresses primarily due to inflation to-the pricing date. Construction costs have steadily increased in the Washington, DC area in recent years, and these increases are expected to continue. The District has agreed to contribute up to 50% of the total project costs of the hospital facility. Howard University will be responsible for the remainder of the project costs, including the medical office building, research facilities, working capital, and the financing costs for its portion of the project. Information on debt servicing arrangementsThroughout the planning process, the University has engaged the services of Goldman Sachs to examine its financing options for the NCMC. Analyses included looking at available and commonly used debt instruments to finance the project and the financing cost implications as a stand-alone and partnership project, taking into account the projected financial performance of the NCMC and the current debt load of involved parties. After reviewing the potential financing options, the University assumed that the FHA Mortgage option would be the optimal alternative. District ContributionThe District is examining several methods of financing for its portion of the hospital costs including:
The District, Howard University and their respective advisors are evaluating these financing alternatives and will present a full financing plan in the Council submission due in the fall of 2005. This financing plan will incorporate a revised project costs estimate, which will be used for purposes of determining the District's contribution. XII. Next stepsThe District and Howard University have already completed most of the planning and analysis necessary for Council to make decisions about the National Capital Medical Center (NCMC) project. The need for the facility has been demonstrated, its services have been defined, and its required size has been estimated. Through the remainder of the summer, the joint District/Howard team will revise project cost estimates and project timeline, and District and Howard officials will complete and sign two major agreements, an Exclusive Rights Agreement (ERA) and a Grant Agreement. By Fall of 2005, the Mayor will introduce legislation for Council action. This will include the signed agreements and a financing package. Starting in 2006, the District will prepare the site for construction by moving existing programs and services, demolishing building, completing any necessary environmental remediation, grading the site, and constructing new streets. In the meantime, the joint team will continue to refine the project design, soliciting input from the community. This will yield a detailed functional space program for the hospital, which will detail all rooms in the facility, including square footage and major requirements. This space program will be a major input to detailed architectural drawings. Any questions or comments on this document or the NCMC project in general should be directed to: The District of Columbia Howard University 1. Kaiser Family Foundation, 2003 2. There are currently estimated to be 23,688 uninsured residents above 200% of the federal poverty level. More than one-third of the individuals in this group (9243) are above 400% of the federal poverty level. Source: Urban Institute analysis based on 2001-2003 Current Population Survey Data. 3. Cumulative enrollment of unique individuals over the course of FY04, Healthcare Safety Net Administration 4. Income Maintenance Administration 5. A medical home is a primary care community health center serving lower income people where a patient’s health history is known, where he or she will be seen regardless of ability to pay, and where he or she routinely seeks non-emergency care. 6. Variance from projections based on historical utilization. Source: Healthcare Safety Net Administration. 7. An avoidable hospitalization is defined as an admission for an ambulatory care sensitive condition such as asthma, diabetes or heart disease, which could have been prevented with adequate primary care. RAND Corporation analysis sponsored by the DC Primary Care Association. 8. The Alliance program is currently a contract between the District Government and five different healthcare organizations. In addition, many other providers participate in the Alliance through subcontracts. Administration, including eligibility and claims-processing, is handled separately from the Medicaid program. The current reform effort aims to integrate the Alliance with the Medicaid Managed Care program such that the District can improve health outcomes, maximize federal revenues, and create a more seamless program for enrollees. 9. Regular source of care is defined as a primary care physician, community health center or outpatient hospital department. Source: RAND Corporation analysis sponsored by the DC Primary Care Association. 10. The first round of Medical Homes capital grants will be awarded by the DC Primary Care Association to nonprofit community health centers in September 2005. This will begin a comprehensive capital planning process for a number of new health center projects around the District. 11. Medical Homes standards were published in spring of 2005 by the DC Primary Care Association and certification processes, including technical assistance for health centers seeking to improve their performance, will begin in 2006. 12. District of Columbia Hospital Association 13. Stroudwater Associates
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()
Send mail with questions or comments to webmaster@dcwatch.com
Web site copyright ©DCWatch (ISSN 1546-4296)

{kind=link}